This blog is a critical appraisal of the following randomized controlled trial: Responsiveness of Myofascial Trigger Points to Single and Multiple Trigger Point Release Massages
Background
During a recent Musculoskeletal (MSK) placement, I encountered the use of trigger point therapy for treatment of a skeletal muscle disorder characterised by regional muscular pain (myofascial pain syndrome [MPS]).
Myofascial trigger points (MTrPs) are nodules in a tight band of skeletal muscle which have an exaggerated response to moderate stimuli. These MTrPs are present in patients with MPS. In tension-type headache (TTH), a type of MPS, MTrPs in the cervical muscles have been identified as potential treatment sites for pain reduction (Fernández-de-las-Peñas et al., 2011). However, placebo-controlled studies on the effect of multiple sessions of massage on MTrPs are currently lacking.
Study Methods
The aim of this study was to assess changes in MTrP pressure-pain threshold (PPT) after single and multiple massage interventions at two muscles in patients with TTH. A total of 69 subjects were screened against eligibility criteria, with 7 subjects excluded; therefore, 62 subjects were randomised. The study subjects were assigned to treatment using block randomisation and the study statistician was blinded to group allocation.
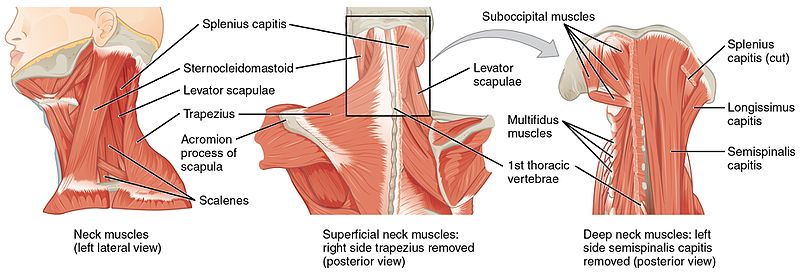
The intervention was twice-weekly massage for 6 weeks, which was compared to sham ultrasound for 6 weeks or wait-list control. In each subject, MTrPs were identified by massage therapists using published criteria and the PPT of the bilateral upper trapezius and suboccipital muscles was assessed before and after the first and last intervention sessions or at a time-matched period for the wait-list control group. The primary outcome measure was algometric assessment of PPT at a MTrP.
Study Results
This study showed that single and multiple massage applications increased PPT at MTrPs when compared to placebo or wait-list control interventions in subjects with TTH. Additional gain in PPT was observed even after multiple massage treatments, suggesting that the number and length of massage treatments needs to be optimised.
Critical Appraisal of Study
The strengths and weaknesses of the study design and the value of the evidence were assessed using the Critical Appraisal Skills Programme (CASP) randomised controlled trial tool as a basis to guide the appraisal. The study population, intervention and control groups, study endpoints, and assessments used were clearly outlined. In addition, the study protocol was registered with ClinicalTrials.gov which shows that the researchers were transparent in their methods and used a standardized protocol.
In order to reduce selection bias between the treatment groups, block randomisation was used. This also ensured that equal numbers of patients were assigned to each treatment group, which is particularly important when the sample size is small (Efird, 2011). Another commonly used method to reduce bias is the concealment of treatment group allocation through blinding (Karanicolas, et al., 2010). In this study, patients and therapists were not blinded to treatment group due to the nature of the interventions. However, the patients and the nurses performing the placebo control ultrasound were blinded to the sham nature of the technique. Also, the statisticians who analysed the outcome data were blinded to treatment group assignment. Thus, although this was not a fully blinded study, measures were taken to minimise bias during data analysis.
The main limitation of this study is that the sample size was very small. Although there was a statistically significant increase (p<0.05) in PPT in the massage intervention group, it cannot be concluded with any certainty that the same results would be obtained in a larger population. A small local sample of the TTH population is not necessarily truly representative of the wider global population of patients with this condition.
The primary endpoint of change in PPT was measured using an algometer, which is a validated technique (Kinser, et al., 2009), particularly when study staff are trained in its use as they were in this study. However, pain is always very subjective and so difficult to accurately measure. The researchers tried to control for changes in pain sensitivity over time by also measuring PPT on the tibia of each patient, and demonstrated no significant change. While change in PPT is a relevant and valid endpoint, a more pertinent question may have been whether massage therapy actually improved TTH symptoms, which was not addressed in this study. Perhaps this could have been included as a secondary endpoint.
Conclusions
This well-designed study clearly achieved its objective by showing a statistically significant effect of massage therapy on PPT of MTrPs. However, the evidence is not currently robust enough to lead to changes in clinical practice. Further studies are needed to test this technique on larger populations so that a systematic review of the overall evidence can be performed.
References
The post Responsiveness of Myofascial Trigger Points to Single and Multiple Trigger Point Release Massages: A critical appraisal appeared first on Students 4 Best Evidence.
No comments:
Post a Comment