Make your goals measurable, achievable, and have an end in sight. You've got this.
The post How to Win at Your 2018 Money Goals appeared first on Earnest Blog | Money Advice for Young Professionals.
Make your goals measurable, achievable, and have an end in sight. You've got this.
The post How to Win at Your 2018 Money Goals appeared first on Earnest Blog | Money Advice for Young Professionals.
Three years after I started my journey, I successfully paid off approximately $54,000 of debt. Here are the strategies that helped me achieve debt freedom.
The post How I Paid Off $54,000 in Debt appeared first on Earnest Blog | Money Advice for Young Professionals.
In the October 2017 Canadian Agency for Drugs and Technologies in Health (CADTH) webinar lecture series, Dr. Hakique Virani presented “Canada’s Opioid Crisis: The Changing Reality Between Exam Rooms and Ivory Towers”. Here, Virani discussed the history, complexities, and current state of the Canadian opioid crisis, outlining a striking metaphor for the way in which researchers have struggled to explain its causes and outcomes.
Midway through the lecture, Virani plays a video of two teams clad in black and white jerseys, each passing a basketball between them. “You are responsible for keeping an eye on the ball carried by the white team and counting how many passes that white team makes”. At the end of the video he asks the audience for the number – “Did everyone get 13?” Following a muffled yes from the crowd, he continues, “Okay. Did you see the moon-walking bear?” At first there is a quiet laugh at the absurdity of the question. But low-and-behold, when the video is played again, a man dressed as a bear walks into the centre of the frame and begins to moonwalk. It had been there the whole time, we just missed it. And why? “It’s easy to miss something you’re not looking for” (1).
With this metaphor, Virani describes what he perceives as an overemphasis on opioid prescribing in research addressing the epidemic. The passing of the ball symbolizes prescription opioid data, the audience symbolizes Canada’s researchers investigating the crisis, and the dancing bear symbolizes the truth underlying the rise in addiction and overdose. According to Virani, researchers have been so preoccupied with establishing links between the crisis and prescribing data that they have missed the real-time changes in opioid-related deaths.
That is, what is the information that we’re missing to aid us in understanding the stark rise in overdose in the last 5 years? Virani seems to suggest that the answer lies in moving away from the investigation of prescripton opioids. But perhaps it doesn’t (at least not entirely). Researchers may simply need to shift exactly what questions about prescription opioids they’re asking.
It is no secret that with the rise of the opioid crisis, there has been a rise in opioid prescriptions, and Virani acknowledges this. It has been found that physicians who prescribe more opioids are more likely to have prescribed the final opioid before an individual’s overdose death (2), that deaths from opioid overdose are more common in areas where opioids are more often prescribed (2-4), and that higher-doses and longer durations are correlated with increased drug-related mortality (5,6). Moreover, recent data suggests that prescriptions in Canada are continuing to increase (7). It is no question that opioid prescribing is tied to the Canadian opioid crisis (8). The question that might be missed, however, is how. As many links have been established between opioid prescribing and addiction, it is still uncertain exactly how prescriptions are having this impact.
This question is particularly confusing in light of the reported low rates of addiction amongst patients actually prescribed opioids (9). A 2012 systematic review found that a mere 0.5% of all opioid-prescribed patients developed an addiction (10). Other reviews have found incidences ranging from 0.8-26% (11).
There are a number of plausible answers to this question: diversion (8, 12), inadequate pain care (13), premature discontinuation of prescription opioids (14), doctor shopping (12) – however, research has not adequately examined which of these avenues is playing the greatest role in exacerbating the observed rise in addiction and overdose.
We need reviews aimed at investigating the primary ways in which prescription opioids enter and influence the lives of not only those who are prescribed opioids, but those that are not. These investigations are particularly important if we hope to introduce policy, programs, and healthcare training that effectively balance the need for improved pain care and safe opioid prescribing. Researchers need to refocus their attention onto this moon-walking bear.
The post Prescription opioids and Canada’s opioid crisis: A call for broadened research appeared first on Students 4 Best Evidence.
If you’ve gotten by without it for this long, do you really need it?
The post Is renters insurance worth it? appeared first on Earnest Blog | Money Advice for Young Professionals.
Case-control and cohort studies are observational studies that lie near the middle of the hierarchy of evidence. These types of studies, along with randomised controlled trials, constitute analytical studies, whereas case reports and case series define descriptive studies (1). Although these studies are not ranked as highly as randomised controlled trials, they can provide strong evidence if designed appropriately.
Case-control studies are retrospective. They clearly define two groups at the start: one with the outcome/disease and one without the outcome/disease. They look back to assess whether there is a statistically significant difference in the rates of exposure to a defined risk factor between the groups. See Figure 1 for a pictorial representation of a case-control study design. This can suggest associations between the risk factor and development of the disease in question, although no definitive causality can be drawn. The main outcome measure in case-control studies is odds ratio (OR).
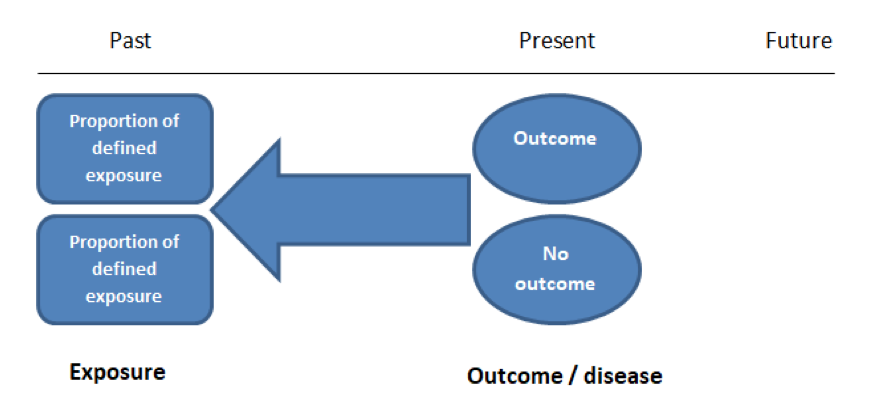
Figure 1. Case-control study design.
Cases should be selected based on objective inclusion and exclusion criteria from a reliable source such as a disease registry. An inherent issue with selecting cases is that a certain proportion of those with the disease would not have a formal diagnosis, may not present for medical care, may be misdiagnosed or may have died before getting a diagnosis. Regardless of how the cases are selected, they should be representative of the broader disease population that you are investigating to ensure generalisability.
Case-control studies should include two groups that are identical EXCEPT for their outcome / disease status.
As such, controls should also be selected carefully. It is possible to match controls to the cases selected on the basis of various factors (e.g. age, sex) to ensure these do not confound the study results. It may even increase statistical power and study precision by choosing up to three or four controls per case (2).
Case-controls can provide fast results and they are cheaper to perform than most other studies. The fact that the analysis is retrospective, allows rare diseases or diseases with long latency periods to be investigated. Furthermore, you can assess multiple exposures to get a better understanding of possible risk factors for the defined outcome / disease.
Nevertheless, as case-controls are retrospective, they are more prone to bias. One of the main examples is recall bias. Often case-control studies require the participants to self-report their exposure to a certain factor. Recall bias is the systematic difference in how the two groups may recall past events e.g. in a study investigating stillbirth, a mother who experienced this may recall the possible contributing factors a lot more vividly than a mother who had a healthy birth.
A summary of the pros and cons of cohort studies are provided in Table 2.
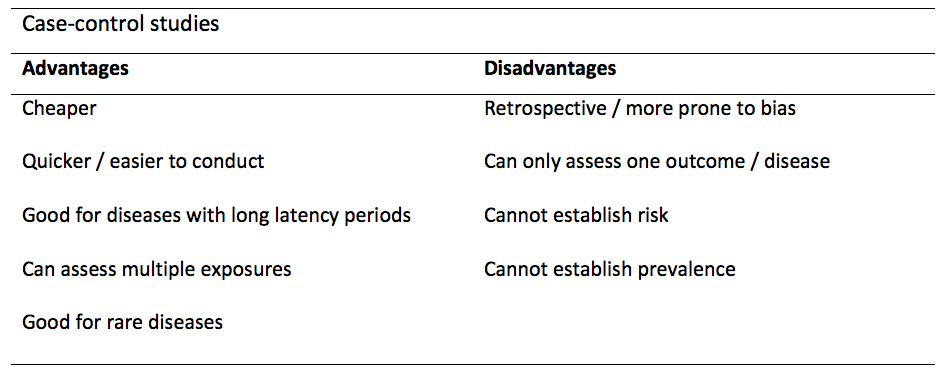
Table 1. Advantages and disadvantages of case-control studies.
Cohort studies can be retrospective or prospective. Retrospective cohort studies are NOT the same as case-control studies.
In retrospective cohort studies, the exposure and outcomes have already happened. They are usually conducted on data that already exists (from prospective studies) and the exposures are defined before looking at the existing outcome data to see whether exposure to a risk factor is associated with a statistically significant difference in the outcome development rate.
Prospective cohort studies are more common. These studies define an exposure and recruit participants into two groups – those that have been subjected to it and those that have not. The study then follows these participants for a defined period to assess the proportion that develop the outcome/disease of interest. See Figure 2 for a pictorial representation of a cohort study design. Therefore, cohort studies are good for assessing prognosis, risk factors and harm. The outcome measure in cohort studies is usually a risk ratio / relative risk (RR).
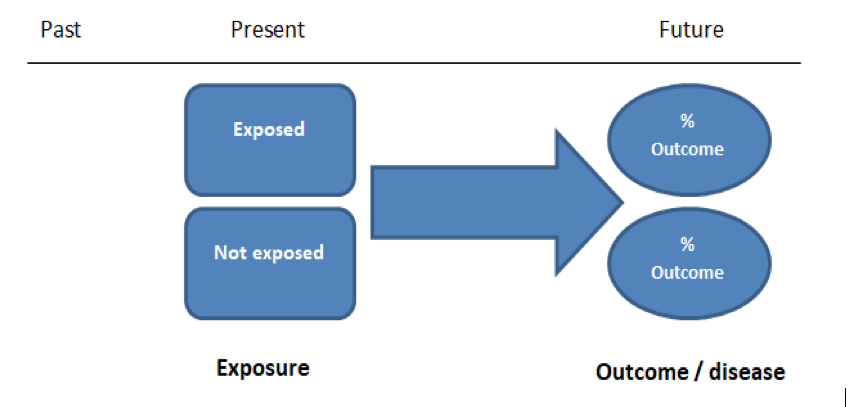
Figure 2. Cohort study design.
Cohort studies should include two groups that are identical EXCEPT for their exposure status.
As a result, both exposed and unexposed groups should be recruited from the same source population. Another important consideration is attrition. If a significant number of participants are not followed up (lost, death, dropped out) then this may impact the validity of the study. Not only does it decrease the study’s power, but there may be attrition bias – a significant difference between the groups of those that did not complete the study.
Cohort studies can assess a range of outcomes allowing an exposure to be rigorously assessed for its impact in developing disease. Additionally, they are good for rare exposures, e.g. contact with a chemical radiation blast.
Whilst cohort studies are useful, they can be expensive and time-consuming, especially if a long follow-up period is chosen or the disease itself is rare or has a long latency.
A summary of the pros and cons of case-controls are provided in Table 1.
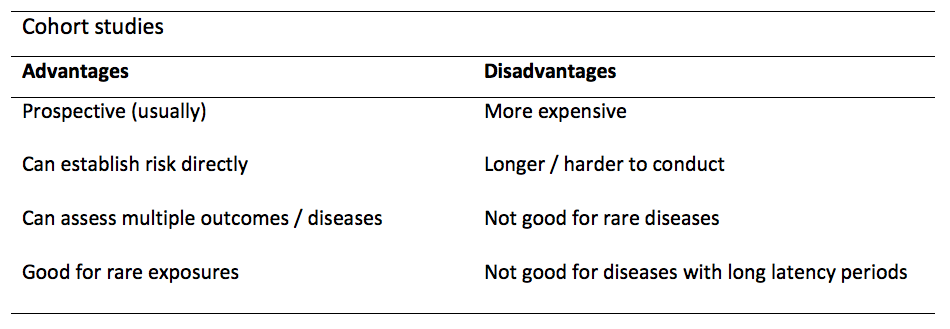
Table 2. Advantages and disadvantages of cohort studies.
STROBE provides a checklist of important steps for conducting these types of studies, as well as acting as best-practice reporting guidelines (3). Both case-control and cohort studies are observational, with varying advantages and disadvantages. However, the most important factor to the quality of evidence these studies provide, is their methodological quality.
The post Case-control and Cohort studies: A brief overview appeared first on Students 4 Best Evidence.
Misdiagnosis – a medical error that leads to no treatment or simply incorrect treatment. How does this impact kids-especially little-gifted ones? In today’s fast-paced world, parents have no patience, or time to read, understand and educate themselves on facts that could change a kid’s life forever. Everyone looks for quick fixes, whether it’s home, workplace, or their own child. If a kid tends to have a restless personality, a general mentality would be to get a quick fix by dropping into physician’s office; taking the diagnosis at face value, and starting the kid on medication. No one today has time to dwell in depth on the causes of certain behaviors, leave alone giving much thought to the side effects of medication given to kids.
Attention Deficit Disorder (ADD), and Attention Deficit/Hyperactivity Disorder (ADHD) are medical terms that are often used interchangeably, although the current correct medical terminology is ADHD or Attention Deficit/Hyperactivity Disorder. ADHD- a highly genetic, brain-based syndrome has to do with the regulation of a particular set of brain functions and related behaviors. “These brain operations are collectively referred to as “executive functioning skills” and include important functions such as attention, concentration, memory, motivation, and effort, learning from mistakes, impulsivity, hyperactivity, organization, and social skills”(Attention Deficient Disorder Association [ADDA],n.d).
Characteristics of gifted kids are frightfully similar. High degrees of intensity, sensitivity, and overexcitability are characteristics that most gifted children have in common. “They may love movement for its own sake and show a surplus of energy exhibited by rapid speech, wild enthusiasm, intense physical activity, and a need for action. This behavior can be misdiagnosed as ADD/ADHD” (Carlstrom,2011,para.5).
More information on possible problems that may be associated with characteristic strengths of gifted children, can be found in article “Misdiagnosis and Dual Diagnosis of Gifted Children” (J.Webb, Amend, N.Webb, Goerss, Beljan & Olenchak,2011, para.10)
In order to give your child a life they deserve; you need to become their first advocate. Follow the tips below to avoid misdiagnosis:
Misdiagnosis can be devastating, altering a child’s life forever. Being exceptional is a “gift” from nature, which demands adequate nurturing. If left unattended, and misdiagnosed; it becomes self-destructive, and a “talent” wasted.
Watch the SENG video: The Misdiagnosis of Gifted Children, for more information.
The post Misdiagnosis – Impact On Gifted Kids appeared first on .
In this blog I want to explore the question of what moral values underpin or justify the practice of evidence-based medicine (EBM). For example, we might be interested in patient outcomes, patient choice, economic factors, public health, or a combination of these. It matters because this provides the standard for evaluating the success of EBM, and informs us about how we can make EBM better. In particular, I want to respond to a recent paper by Anjum and Mumford on ‘A philosophical argument against EBM’ [1], which argues that the values underpinning EBM inevitably collapse.
Utilitarianism is the view that, when faced with a moral dilemma, we ought to act according to which of our options causes the greatest amount of overall wellbeing or happiness, and the least amount of suffering. Rule utilitarianism specifically looks at which rules, heuristics or policies are able to do this, rather than looking at each action individually [2]. In the context of medicine, this means we should aim to create healthcare policies which promote the best standard of health for the greatest number of patients.
An important aspect to this approach is that these policies do not always create the best possible benefit for the patient. In some cases, the guidelines will be ineffective. For example, a given treatment may be recommended in general cases of patients with an illness, but in the case of a particular patient we know it would be harmful. It’s just that having this policy in place for all patients is worthwhile overall. How we respond to such scenarios poses a problem for the rule utilitarian.
Here, we might still say that the treatment recommendation is a good guideline (because it maximises patient health) but in this case, it would seem unethical to prescribe the treatment in the knowledge that it will cause harm. We therefore probably want to say that even good evidence-based guidelines have exceptions. However, this risks compromising the whole point of rule utilitarianism – if we have a set of rules which determine how we should act, but we can contradict or find exception to these rules whenever we need to, what’s the point of having those rules at all? It seems we haven’t said anything that won’t dissolve back down into the more general utilitarian principle of maximising health, regardless of what rules/policies we create [3].
This way, policies which are based on EBM can offer us guidance for how a practitioner should act, but nonetheless require a practitioner to use their own judgement and common sense in applying them.
I want to respond to this paper by contesting the authors’ initial premise that EBM implies a kind of rule utilitarianism. I would suggest that, if we seriously look at our medical policies, conventions and laws, the picture is in reality far more complicated than this.
To see why this is the case we need to bear in mind that utilitarianism is not the view that ‘consequences matter’. Everyone cares about what the outcomes of their actions are, and pretty much everyone agrees that it’s generally better to cause happiness rather than suffering. What makes utilitarianism unique is the view that only these consequences matter, meaning there are no values that should influence our actions other than the impact that the action will have on other peoples’ lives. For example, this suggests that there is nothing wrong with lying, coercion, torture or manipulation, except for the fact that they can have bad consequences.
Whether these non-utilitarian values should have any significance from a moral perspective is beyond the scope of this article.
An adult patient requires medication for a fatal illness that they are at significant risk of contracting. However, due to their religious beliefs they refuse to take this medication because it contains an ingredient derived from animals. This refusal is clearly bad for them – they have a high chance of dying if they don’t take the medication. A week after the patient saw her doctor and refused to take this medication, she has a small accident and is taken to hospital unconscious.
In a stroke of luck, the same doctor who saw her a week before is passing her ward. The doctor knows the patient’s medical history and knows there is no chance of the patient having an adverse reaction to the medication which she refused. The doctor (a utilitarian) decides to take the opportunity, while the patient is unconscious and while there are no other patients around, to administer the medication to her, without her consent. The doctor has done something good for the patient – she has potentially saved her life, and there is no chance of being found out.
I hope we would agree that in this case the doctor has done something unethical. She has clearly ignored the patient’s own wishes and values, violated her right to consent and openly deceived her. Of course, a rule utilitarian could always avoid stating the uncomfortable conclusion that the doctor was ethical by deferring to policies – it’s better for everyone if we have policies and regulations against doctors deceiving patients, for example. This conclusion seems pretty unsatisfactory however. This suggests that the only reason this doctor’s actions are unethical is because she has violated hospital regulations. There would be nothing wrong, in this view, with creating a law which allowed doctors to deceive patients if only it had desirable consequences for the overall health of patients.
What’s ultimately at issue here is the patient’s right to decide how to live her own life – according to her own values, judgements and preferences, which may not always align with a medical model of what a healthy patient looks like. The role of the doctor is not to decide on a set of desirable outcomes for the patient and enforce them on her; rather, it should be to help the patient to determine her own ends, insofar as her health affects this.
These non-utilitarian values also play a role in the literature on EBM specifically. For example, an article from the Evidence-Based Medicine Working Group in 1992 defends EBM on the grounds that it gives patients a clearer understanding of their prognosis, diagnosis and treatment/s [5]. According to their argument, deferring to clinical intuition or expertise, risks leaving patients “in a state of vague trepidation” about their health prospects and choices. By contrast, the openness about evidence which EBM encourages, offers the patient a more transparent picture of their expected outcomes and options. EBM in this way doesn’t just aim at increasing positive utilitarian outcomes, it can also have benefits from the perspective of the patients’ rights, autonomy, and choice.
[1] Anjum RL and Mumford SD. A philosophical argument against evidence-based policy: Philosophical argument against EBP. Journal of Evaluation in Clinical Practice. 2017,October;23(5): 1045–1050. doi:10.1111/jep.12578
[2] For an explanation of the difference between act and rule utilitarianism see: Utilitarianism, Act and Rule | Internet Encyclopedia of Philosophy
[3] This is a version of an argument by Smart. Smart JCC (1973) An outline of a system of utilitarian ethics. In Utilitarianism: For and Against (eds J. C. C. Smart & B. Williams), pp. 1–74. Cambridge: Cambridge University Press.
[4] Hooker B. (1995) Rule-consequentialism, incoherence and fairness. Proceedings of the Aristotelian Society;95:19–35.
[5] Guyatt G, Cairns J, Churchill D, et al. Evidence-Based Medicine A New Approach to Teaching the Practice of Medicine. JAMA. 1992 November;268(17):2420–2425. doi:10.1001/jama.1992.03490170092032
The post Does Evidence-Based Medicine Imply Utilitarianism? appeared first on Students 4 Best Evidence.
In the medical literature, it is very common to find variables associated with a specific outcome. For example, increased body mass index (the variable) might be associated with an increased risk of cancer (the outcome). However, an association does not always imply that one thing caused the other. It’s important to consider other possible interpretations.
Here are the 5 interpretations that you should consider when you read or hear about a reported association in observational studies:
The relationship between the variable and the outcome occurred by chance.
What’s really happening? There is no true association. It may be that two events appear to be related, just by coincidence.
Clues that this might be the case: The results can’t be replicated by repeating the study. We need to view the precision of the reported association.
For example, you find a reported association between watching TV and myopia in an observational study. However, at the time that you conduct a similar study you found no association, therefore the association could have occurred by chance.
There is no true cause-and-effect relationship, there just appears to be. However, the results are not due to chance, but due to bias.
What’s really happening? There are issues in the design and application of the study which give a false impression that there is a relationship between the variable and outcome of interest.
Clues that this might be the case: The results are inconsistent with other similar studies; there may be issues of bias in the study design or conduct (e.g. confounders), or in the analysis of the results. “The greater the error the less accurate the variable”.
For example, you found an association between vaginal breech delivery and developmental dysplasia of the hip. However, the paediatrician’s examination was more detailed in newborns with breech presentation than those with cephalic presentation. There could be a diagnosis bias, in which certain perceptions alter the probability of diagnosing a certain disease between groups.
There really is a causal relationship, but in the opposite direction from that reported, meaning that the interpretation of the relationship is incorrect.
What’s really happening? The supposed outcome is the real cause, and the supposed cause is the real outcome.
This can be a problem in study designs that don’t address temporality, e.g. cross-sectional and case-control studies.
For example, if you were to identify a relationship between taking non-steroidal anti-inflammatory drugs (NSAIDs) and a greater risk of spontaneous abortion, you may think that the NSAIDs caused the spontaneous abortion. However, it is also possible that the NSAIDs could be taken to relieve the pain due to early symptoms of the spontaneous abortion itself. This misunderstanding is known as protopathic bias (when a drug is initiated in response to the first symptoms of a disease which is, at this point, undiagnosed).
There is an unmeasured variable which explains the association.
What’s really happening? There is an unknown variable that intervenes in the relation, it could be between the “cause” and the “effect”, or a single variable causes both “cause” and “effect”.
For example, if you were to identify a relationship between having a higher BMI and a greater risk of cancer, you might think that having a high BMI causes cancer. However, it would be important to consider whether other factors associated with having a higher BMI (e.g. poorer diet, less physical activity) could explain the increased cancer risk.
There really is a cause-effect relationship.
You could also go further and evaluate your causality (e.g. using the Bradford Hill criteria; a set of principles for assessing the likelihood that there is a causal relationship between a presumed cause and effect):
Hulley SB, Cummings SR, Browner WS, Grady DG and Newman TB (2013). Designing clinical research. Lippincott Williams & Wilkins.
Swaen G and van Amelsvoort L (2009). A weight of evidence approach to causal inference. Journal of clinical epidemiology; 62(3):270-277.
The post Assessing associations in observational studies appeared first on Students 4 Best Evidence.